
- Registrado
- 16 Mar 2013
- Mensajes
- 7.584
- Calificaciones
- 26.300
Os ofrezco una reflección:
es sabido que entre los efectos adversos de los pinchazos están los leves (vómitos, diarrea, dolor de cabeza, mareos, fiebre, dificultad en caminar, tremores) y los severos (muerte, parálisis, síndrome de Guillaine Barré, tachicardia, miocardios, Herpes Zoster https://onlinelibrary.wiley.com/doi/full/10.1111/jocd.14470, malformaciones congénitas, Thrombocytopenia (numero muy restringido de plaquetas) (https://pubmed.ncbi.nlm.nih.gov/34266487/ https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-05-12/07-COVID-Shimabukuro-508.pdf) y Tr. purpura https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7996471/ ,
Curioso que entre los síntomas producidos por envenenamiento de metales pesados, el arsénico cual metaloide incluido están, están entre otros, los mismos:
por ejemplo
síndrome de Guillaine Barré:

 pubmed.ncbi.nlm.nih.gov
Thrombocytopenia:
pubmed.ncbi.nlm.nih.gov
Thrombocytopenia:
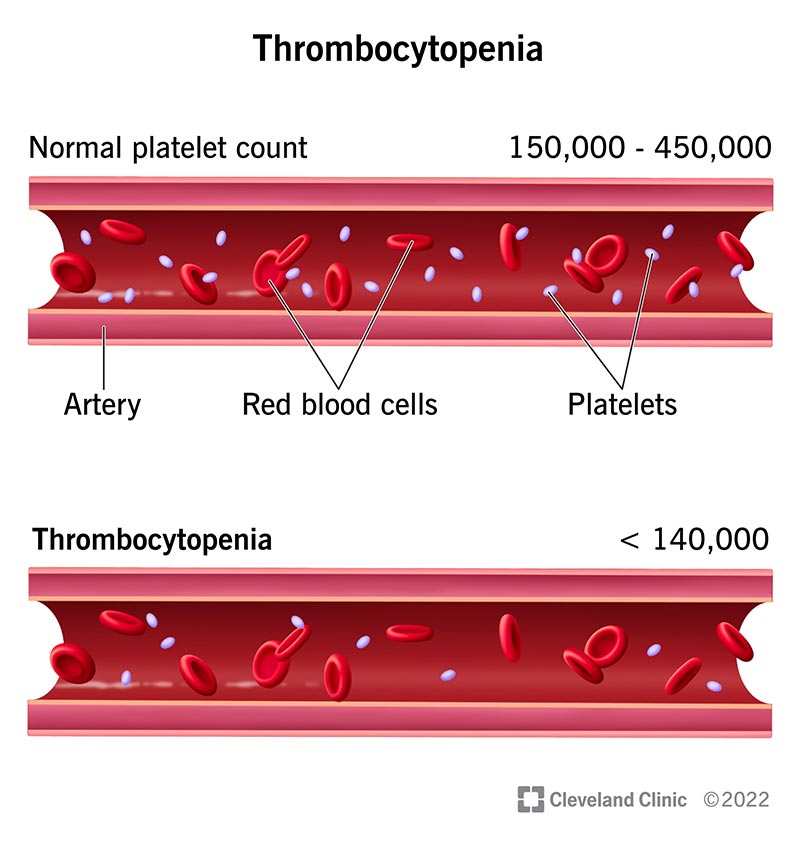
 my.clevelandclinic.org
Herpes Zóster:
my.clevelandclinic.org
Herpes Zóster:
pubmed.ncbi.nlm.nih.gov
A mi suegra, post pinchazo con la anti-gripal en Noviembre le salieron en la cara unas cosas raras, y post Pfizer en marzo-abril se le dispararon. Se parecen mucho a lo que pasa con la enfermedad de Bowen, provocada, entre otros, por envenenamiento con arsénico:

No digo que es lo que ha pasado (que en la inyección de la vacuna para la gripe y la del covid esté incluido el trióxido de arsénico, forma más letal y usada en la medicina desde hace una vida para el tratamiento de algunos tipos de cáncer), pero me choca la coincidencia de síntomas que veo a mi alrededor que aparecen en las personas con sistema inmune debilitado y los inducidos por elementos tóxicos (mareos, debilidad en las extremidades, insomnio, herpes zoster, taquicardia, keratosis...etc, etc)
lo importante es que en el caso de envenenamiento, los daños son cumulativos ( más toxinas introducidas en el organismo, menos posibilidad de deshacerse de ellas) y muchas de las veces quedan mal-diagnosticadas. Me acuerdo de los personages de Agata Christie...y también de las tropeciantas mil dosis que se preparan poner al mundo mundial pretexto covid...
es sabido que entre los efectos adversos de los pinchazos están los leves (vómitos, diarrea, dolor de cabeza, mareos, fiebre, dificultad en caminar, tremores) y los severos (muerte, parálisis, síndrome de Guillaine Barré, tachicardia, miocardios, Herpes Zoster https://onlinelibrary.wiley.com/doi/full/10.1111/jocd.14470, malformaciones congénitas, Thrombocytopenia (numero muy restringido de plaquetas) (https://pubmed.ncbi.nlm.nih.gov/34266487/ https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-05-12/07-COVID-Shimabukuro-508.pdf) y Tr. purpura https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7996471/ ,
Curioso que entre los síntomas producidos por envenenamiento de metales pesados, el arsénico cual metaloide incluido están, están entre otros, los mismos:
por ejemplo
síndrome de Guillaine Barré:
Acute arsenic intoxication presenting as Guillain-Barré-like syndrome - PubMed
Arsenic-induced polyneuropathy is traditionally classified as an axonal-loss type, electrodiagnostically resulting in low amplitude or absent sensory and motor responses, relatively preserved proximal and distal motor conduction rates, and distal denervation. We report four patients with a...
pubmed.ncbi.nlm.nih.govThrombocytopenia: Symptoms, Stages & Treatment
Thrombocytopenia occurs when your bone marrow doesn’t make enough platelets. Platelets form blood clots to help stop bleeding.
Arsenic trioxide therapy predisposes to herpes zoster reactivation despite minimally myelosuppressive therapy - PubMed
Acute Promyelocytic Leukemia (APL) is a unique subtype of acute myeloid leukemia that is highly responsive to minimally myelosuppressive therapy with all-trans retinoic acid (ATRA) and arsenic trioxide (ATO). We and others have observed a higher than expected incidence of herpes zoster...
pubmed.ncbi.nlm.nih.govA mi suegra, post pinchazo con la anti-gripal en Noviembre le salieron en la cara unas cosas raras, y post Pfizer en marzo-abril se le dispararon. Se parecen mucho a lo que pasa con la enfermedad de Bowen, provocada, entre otros, por envenenamiento con arsénico:
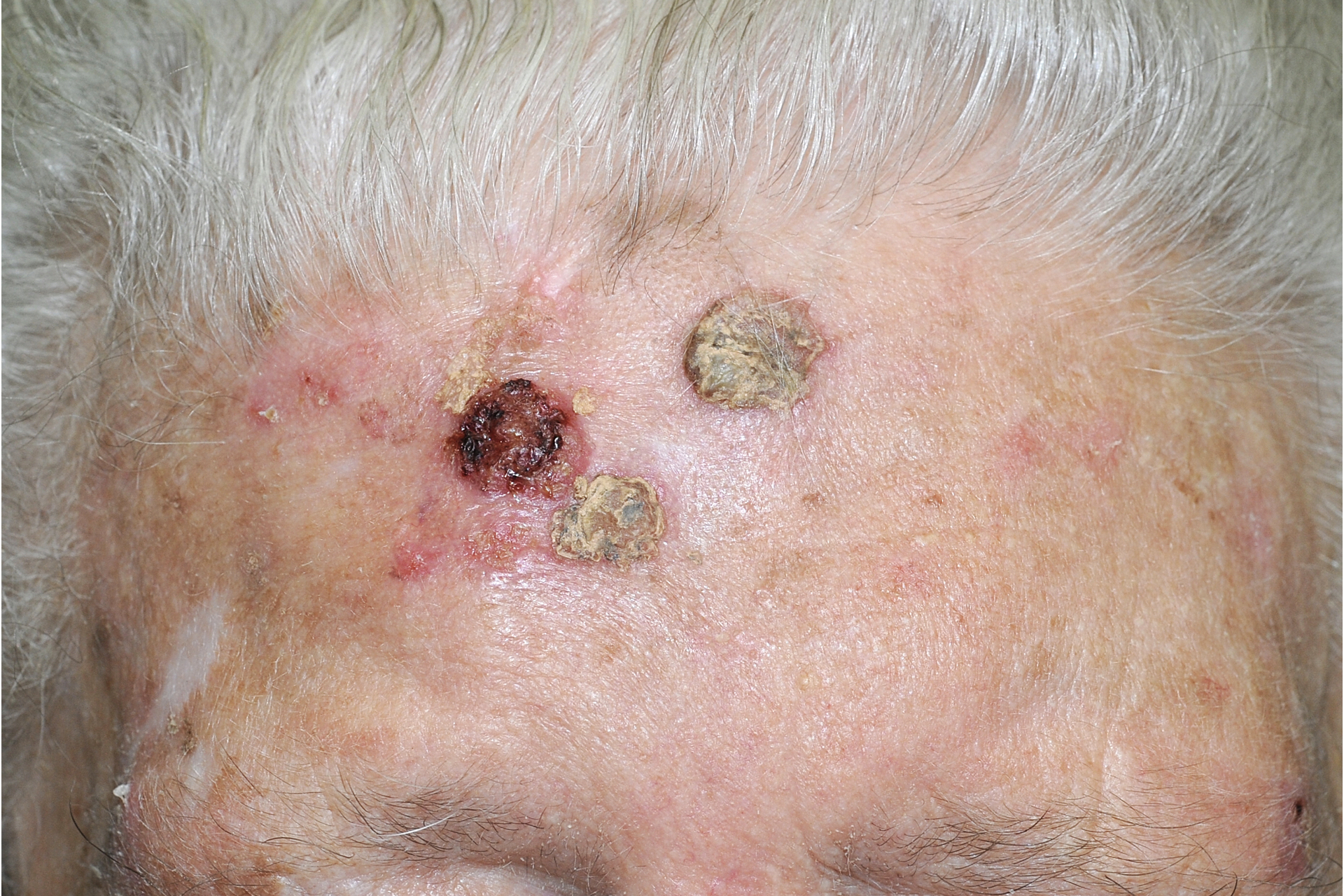
No digo que es lo que ha pasado (que en la inyección de la vacuna para la gripe y la del covid esté incluido el trióxido de arsénico, forma más letal y usada en la medicina desde hace una vida para el tratamiento de algunos tipos de cáncer), pero me choca la coincidencia de síntomas que veo a mi alrededor que aparecen en las personas con sistema inmune debilitado y los inducidos por elementos tóxicos (mareos, debilidad en las extremidades, insomnio, herpes zoster, taquicardia, keratosis...etc, etc)
lo importante es que en el caso de envenenamiento, los daños son cumulativos ( más toxinas introducidas en el organismo, menos posibilidad de deshacerse de ellas) y muchas de las veces quedan mal-diagnosticadas. Me acuerdo de los personages de Agata Christie...y también de las tropeciantas mil dosis que se preparan poner al mundo mundial pretexto covid...
Última edición:
")
